An advanced minimally invasive technique for colorectal cancer
Until recently, many patients with precancerous growths or early cancers of the rectum had to undergo open surgery with a long recovery period and risk of complications. Transanal endoscopic microsurgery (TEM) can eliminate the need for major surgery for many of these patients.
West Chester Hospital is one of the few hospitals in the nation to offer TEM, a minimally invasive option for the removal of certain rectal polyps and early stage rectal tumors. This technique allows patients to recover more quickly with a decreased likelihood of complications than that of major surgery.
 Performed with specially designed equipment, TEM has made it possible to remove tumors high inside the rectum that otherwise would be accessible only through invasive, open abdominal surgery. The patient benefits of TEM, as compared to radical abdominal surgery, include:
Performed with specially designed equipment, TEM has made it possible to remove tumors high inside the rectum that otherwise would be accessible only through invasive, open abdominal surgery. The patient benefits of TEM, as compared to radical abdominal surgery, include:
- Elimination of invasive surgery
- No large incision or stitches
- Reduced risk of infectionNo colostomy
- Less pain
- Faster recovery
- Shorter hospital stay
- Improved quality of life, post-surgery
Traditional Surgery for Colorectal Cancer
There are several types of surgery to remove tumors in the colon and rectum, depending on their location and size. If the tumor is on the inside surface of the intestinal wall, but has not spread into the tissue, the tumor and a small amount of surrounding healthy tissue is removed.
If the cancer has spread into the wall of the colon or rectum, the section of the organ with cancer and the nearby healthy tissue is removed to prevent further spread. Sometimes additional tissue and/or the lymph nodes are removed and inspected for signs of cancer.
Traditionally, these procedures would be done through “radical abdominal surgery,” which involves opening the abdomen and operating from the front of the body. This type of surgery sometimes requires partial removal of the colon, which may have side effects such as permanent colostomy or iliostomy, long-term bladder or erectile dysfunction, and extended recovery time – up to three month in some cases.
About TEM
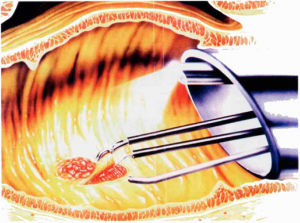
Unlike traditional open surgery, TEM utilizes special equipment to remove colorectal tumors through the rectum. Guided by a video monitor, the surgeon navigates a scope – a thin, flexible instrument equipped with a three-dimensional camera and light at its tip – up through the anal canal to the tumor. This magnifying camera offers significantly improved visualization for the surgeon compared to traditional methods.
The surgeon detaches the tumor and a small section of the surrounding tissue using a specialized electronic scalpel that simultaneously seals affected blood vessels. Once the tumor is removed through the anus, the rectal wall is cleansed and sutured. The procedure, which is performed until general anesthesia, usually takes about an hour.
Because it does not involve cutting open the abdomen, healing time for TEM is nearly immediate. After the operation, the patient can drink and eat right away. In most cases, patients are discharged within 24 hours. Some minor side effects may occur, including pain or temporary incontinence lasting a few days. However, there have been no reported problems of long-term incontinence.
Ask your doctor if you are a candidate for minimally invasive transanal endoscopic microsurgery. Or call (513) 298-DOCS, our toll-free physician referral line, to find a doctor in your area who specializes in TEM.
About Colorectal Cancer
Most cases of colon and rectal (colorectal) cancer begin as small, noncancerous (benign) clumps of cells or polyps in the large intestine or rectum. Polyps may be small and produce few, if any, symptoms. For this reason, doctors recommend regular screening tests to identify polyps, which may lead to the development of colon cancer.
Colon cancer can be diagnosed by a physician through a physical exam, possibly along with a colonoscopy or biopsy – the removal of a small piece of tissue from inside the colon for testing – and/or a blood test that checks for cancer cells in the blood.
Risk factors for colorectal cancer:
- Individuals age 40 or older
- Family history of colorectal cancer or polyps
- Certain hereditary conditions, such as familial adenomatous polyposis (FAP) and hereditary nonpolyposis colon cancer (HNPCC or Lynch syndrome)
- Personal history of colorectal cancer, polyps in the colon or rectum, or cancer of the ovary, endometrium, or breast