
New Program Assesses Cardiovascular Risk In Utero, Cardiologist Nominated as FDA Commissioner
Dear Colleagues,
At the University of Cincinnati Heart, Lung and Vascular Institute, we continue to grow in the areas of cardiovascular research and care by taking our findings and other key insights from the field and translating them into real treatments to help our patients each day. In this issue of Cardiovascular Insights, we highlight some of our most recent discoveries and efforts by our staff to make medical breakthroughs.
Primordial Cardiology and Life Cycles of Cardiovascular Disease:
The HLVI Program for Primordial Cardiology and Life Cycles of Cardiovascular Disease is based on an emerging appreciation that many common cardiovascular conditions, including diabetes, hypertension and coronary heart disease not only have genetic and environmental determinants, but are also impacted by in utero conditions. For example, diabetes during pregnancy increases the risk of diabetes, hypertension and heart disease in the child; typically occurring at an early age and progressing more rapidly than expected. We believe that a predisposition to diabetes, acquired in utero, may, in fact, represent a distinct condition. By investigating and redefining such diseases and medical conditions, the program could develop an entirely new field of study.
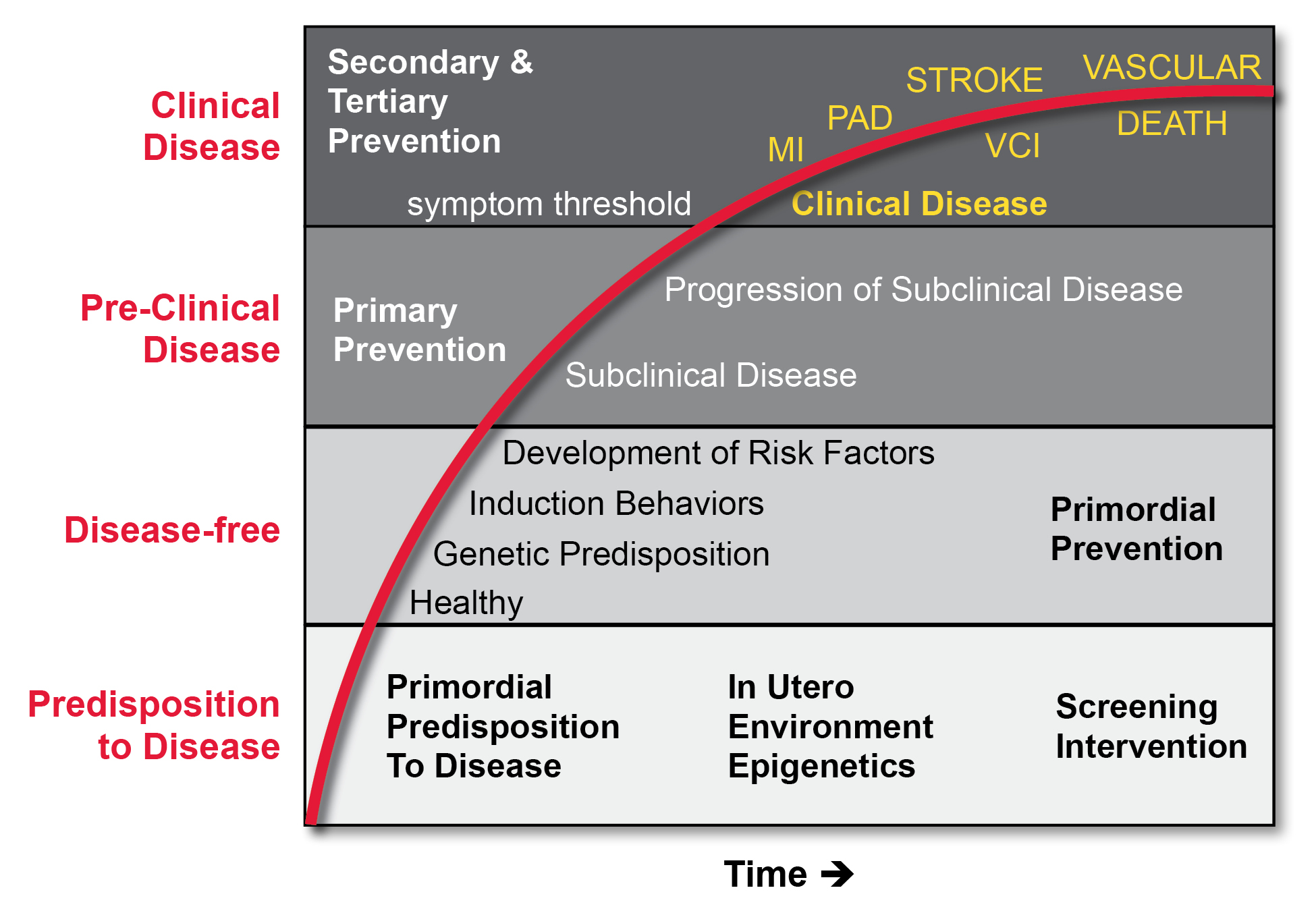
Our recently-initiated Program for Primordial Cardiology and Life Cycles of Cardiovascular Disease, which may be the first of its kind in the country, best demonstrates our commitment to innovation, collaboration and patient-centered care. The program is based on the growing body of evidence that many common cardiovascular (CV) conditions result from not only genetic and environmental factors, but also from in utero conditions. In fact, risk for future atherosclerosis may begin before birth and continue for decades, leading to both nonfatal and fatal cardiovascular events, including myocardial infarction, stroke, and sudden death.1 Clinical trial evidence has shown convincingly that pharmacological treatment of risk factors can prevent events, as can lifestyle changes when adopted early.1
This concept originally arose from observations cited in the obstetrics literature and epidemiology studies reporting that women who had pre-eclampsia or eclampsia during pregnancy or gestational diabetes continued to be at elevated risk of developing CV events compared to age-matched women who didn’t develop these conditions, even after their blood pressure or blood sugar returned to normal levels post-partum. Perhaps most striking is that babies born of these mothers are at higher lifetime risk of CV events themselves. Although the reasons for this in utero risk are not yet fully understood, these findings may herald a major paradigm shift in the field, and could alter the way patient histories are taken, preventive measures are instituted and patients are treated.
Given the newness of this area, our program is just beginning to take shape, and consists of roundtable discussions among adult cardiologists, pediatric cardiologists, obstetricians and maternal/fetal medicine specialists. Recent additions to the group have also included representatives from bioinformatics, a key component as we craft big data approaches, including utilization of de-identified electronic health record (EHR) information and longitudinal assessment of CV events. From a public health perspective, our goal is to respond appropriately to these new data, redefine the natural history of CV disease and implement thoughtful screening and preventive measures.
Just as we are advocates for our patients, we may soon have a strong advocate and visionary leader in the Food and Drug Administration (FDA). We were pleased to learn that a cardiologist, Robert Califf, MD, who is currently working as the FDA Deputy Commissioner for Medical Products and Tobacco, has been nominated by President Obama to serve as the organization’s next Commissioner. I have worked with Dr. Califf for many years, and I’m confident he will bring an excellent understanding of the processes and partnerships needed between the public and private sectors to facilitate medical advances to the betterment of public health.
I hope you will enjoy this issue of Cardiovascular Insights, as you discover more about our innovative and collaborative programs designed to enhance our patients’ treatment experience and our own scientific understanding of the evolving field of cardiovascular medicine.
Sincerely,
Richard C. Becker, MD
Mabel Stonehill Endowed Professor of Medicine
Chief, Division of Cardiovascular Health and Disease
Director and Physician-in-Chief
University of Cincinnati Medical Center Heart, Lung and Vascular Institute
University of Cincinnati College of Medicine
Director, Cardiovascular Services
Reference: 1. Weintraub WS, Daniels SR, Burke LE, Franklin BA, Goff Jr, DC, Hayman LL et al on behalf of the American Heart Association Advocacy Coordinating Committee, Council on Cardiovascular Disease in the Young, Council on the Kidney in Cardiovascular Disease, Council on Epidemiology and Prevention, Council on Cardiovascular Nursing, Council on Arteriosclerosis, Thrombosis and Vascular Biology, Council on Clinical Cardiology, and Stroke Council. Value of Primordial and Primary Prevention for Cardiovascular Disease: A Policy Statement From the American Heart Association. Circulation 2011;124:1-25.

Richard C. Becker, MD
Chief, Division of Cardiovascular Health and Disease
Director and Physician-in-Chief, Heart, Lung and Vascular Institute
Phone: (513) 558-4332
E-mail: beckerrc@ucmail.uc.edu
Leave a reply →