
Developments in Arrhythmia Treatment: Reduced Procedure Time, Planning for Telemedicine
The Arrhythmia Center at the University of Cincinnati (UC) Medical Center, undergoing significant upgrades, is unique in its nationally and internationally recognized electrophysiology group which encompasses strong clinical performance, education and research. Alexandru Costea, MD, professor of medicine, director of the Center for Electrophysiology, Rhythm Disorders and Electro-mechanical Interventions, is leading this multi-faceted cardiac program. The program has distinguished itself not only through an excellent track record of performing complex procedures, but also through fellow education, clinical research and collaboration with world renowned centers of excellence in electrophysiology. Dr. Costea has spearheaded a very successful program of lectures with experts in the field that have been attended by the clinical staff at UC Medical Center as well as electrophysiology and cardiology fellows throughout the country.
Atrial fibrillation (AF) is the most frequently encountered arrhythmia in electrophysiology. Radiofrequency catheter ablation for patients with atrial fibrillation is one procedure that Dr. Costea and his team perform in much less time than in many other medical centers – in 60 to 90 minutes as compared to three to four hours in other national centers. Additionally, “radiation exposure during the procedure is minimal,” says Dr. Costea, “with none or, at most, two minutes of radiation exposure, while the traditional usage of radiation reaches 30 minutes in most other centers. We have set the record with time for ablation and radiation exposure.” Dr. Costea attributes the reduced procedure time and lessened radiation exposure to a standardized protocol and excellence of “a very advanced electrophysiology team.” He estimates that 400 ablation procedures are performed annually at UC Medical Center and the Cincinnati VA Hospital.
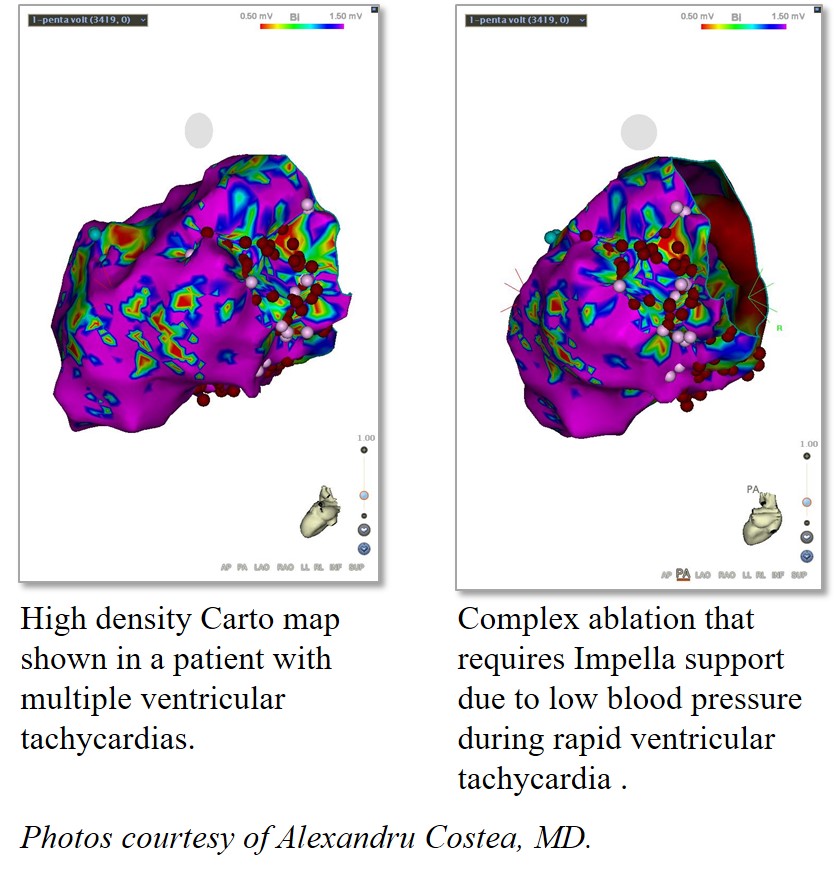 In treating patients with coronary artery disease or advanced heart failure and life-threatening arrhythmias (ventricular tachycardia), Dr. Costea uses an Impella device (Abiomed, Danvers, Mass.) for circulatory support. During these very complex procedures, the risk of critically low blood pressure and even death is very high. Using this temporary cardiac support, which is placed through an artery in the upper portion of the leg, allows the UC Medical Center team to accurately localize the site of arrhythmia, perform an ablation and avoid major complications. Dr. Costea notes that patients experience positive outcomes from this procedure. While before the ablation, most patients had almost incessant life-threatening rhythms and received shocks from their defibrillators, after the procedure, patients experienced no shocks. Dr. Costea notes that the use of the Impella device has become “a standardized approach for very sick patients;” additionally, being able to map and perform ablations on the external surface of the heart (the epicardium) is a necessary adjunct for success in these complex patients.
In treating patients with coronary artery disease or advanced heart failure and life-threatening arrhythmias (ventricular tachycardia), Dr. Costea uses an Impella device (Abiomed, Danvers, Mass.) for circulatory support. During these very complex procedures, the risk of critically low blood pressure and even death is very high. Using this temporary cardiac support, which is placed through an artery in the upper portion of the leg, allows the UC Medical Center team to accurately localize the site of arrhythmia, perform an ablation and avoid major complications. Dr. Costea notes that patients experience positive outcomes from this procedure. While before the ablation, most patients had almost incessant life-threatening rhythms and received shocks from their defibrillators, after the procedure, patients experienced no shocks. Dr. Costea notes that the use of the Impella device has become “a standardized approach for very sick patients;” additionally, being able to map and perform ablations on the external surface of the heart (the epicardium) is a necessary adjunct for success in these complex patients.
Dr. Costea confirmed that discussions are underway with Richard Becker, MD, director and physician-in-chief, UC Heart, Lung, and Vascular Institute, to incorporate telemedicine into patient follow-up. “Electrophysiology is the best area for telemedicine,” says Dr. Costea, because implanted devices “are enabled to send remote transmissions to the UC Medical Center Arrhythmia Center, and we can manage the patients remotely.” According to Dr. Costea, UC Medical Center is in talks to collaborate with a hospital system in Rome, Italy, which also has one of the most effective telemedicine programs in the world.
Upcoming presentation by Alexandru Costea, MD
XVII International Symposium on Progress in Clinical Pacing – Rome, Nov. 29-Dec. 2, 2016.
Ventricular tachycardia ablation: role of implantable monitors
Readings
Costea AI, Platonov PG. Rate modulation drugs in atrial fibrillation: what is the clinical impact? J Cardiovasc Electrophysiol. 2015;26:142-144.
Costea AI. Ventricular tachycardia ablation: are we as successful as we believe we are? J Cardiovasc Electrophysiol. 2016 Sep 13. doi: 10.1111/jce.1309. Accessed September 15, 2016.
Eckman MH, Lip GY, Wise RE, Speer B, Sullivan M, Walker N, Kissela B, Flaherty ML, Kleindorfer D, Baker P, Ireton R, Hoskins D, Harnett BM, Aguilar C, Leonard AC, Arduser L, Steen D, Costea A, Kues J. Impact of an atrial fibrillation decision support tool on thromboprophylaxis for atrial fibrillation. Am Heart J. 2016;176:17-27.
Eckman MH, Lip GY, Wise RE, Speer B, Sullivan M, Walker N, Kissela B, Flaherty ML, Kleindorfer D, Baker P, Ireton R, Hoskins D, Harnett BM, Aguilar C, Leonard A, Arduser L, Steen D, Costea A, Kues J. Using an atrial fibrillation decision support tool for thromboprophylaxis in atrial fibrillation: effect of sex and age. J Am Geriatr Soc. 2016;64:1054-1060.
Zhou Y, Lower EE, Li HP, Costea A, Attari M, Aughman RP. Cardiac sarcoidosis: the impact of age and implanted devices on survival. Chest. 2016 Sep 7. pii: S0012-3692(16)58892-8. doi: 10.1016/j.chest.2016.08.1457. Accessed September 15, 2016.
Impella 2.5 system – P140003 available at http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/DeviceApprovalsandClearances/Recently-ApprovedDevices/ucm442092.htm. Accessed August 10, 2016.

Alexandru Costea, MD
Director for the Center for Electrophysiology, Rhythm Disorders and Electro-Mechanical Interventions
Professor of Medicine
Phone: (513) 558-4721
Email: costeaai@ucmail.uc.edu
Connect with Dr. Costea on Doximity
Leave a reply →