
Advancing the Standard of Care: Fibrinolytic Therapy Facilitated Transradial Percutaneous Coronary Intervention Effective Treatment for Acute STEMI
In the hands of experienced operators and high-volume transradial catheterization centers, transradial coronary angiography and intervention offer improved patient comfort, decreased access-site complications, and lower costs without compromising procedural success or long-term outcomes. Patients presenting with ST-elevation myocardial infarction (STEMI), in particular, benefit from a transradial approach to coronary intervention.

Radial artery access being used to perform transradial cardiac catheterization
The transfemoral approach has remained the primary route of arterial access for cardiac catheterization in the United States. As recently as 2008, only 1.3 percent of coronary interventions were performed via the transradial approach.1 Transradial catheterization is performed more frequently in Europe and Asia.2,3 However, transradial cardiac catheterization in the US has seen growing use and enthusiasm over recent years with mounting data showing clinical benefit, primarily decreased access-site complications, such as post-procedural bleeding. Transradial PCI procedures increased to 16.1 percent in 2012 and accounted for 6.3 percent of total procedures from 2007 to 2012 (n=178,643).4
Case in point: A 40-year-old male patient presented with chest pain to the University of Cincinnati Medical Center. When he arrived in the emergency room, he went into cardiac arrest and underwent prolonged cardiopulmonary resuscitation for more than 45 minutes.
“He underwent defibrillation and shock therapy more than 25 times for incessant ventricular tachycardia and fibrillation,” says Imran Arif, MD, a cardiologist at the University of Cincinnati Medical Center. “If not for aggressive CPR, fibrinolysis, and rapid availability of an experienced heart catheterization team, he probably wouldn’t be alive.”
The emergency department team administered a fibrinolytic therapy, and the patient stabilized briefly before an electrocardiogram showed he was having an anterior wall STEMI. “We took him from the ER to the cardiac catheterization lab room and did an emergency angiography and percutaneous coronary intervention via transradial approach,” explains Arif.
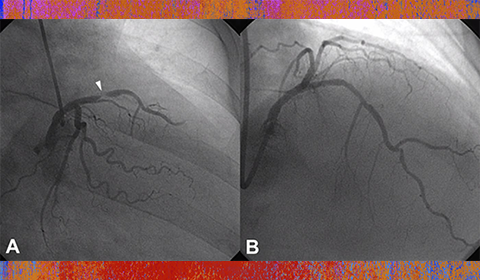
The patient had a critical 99 percent stenosis in the middle left anterior descending artery with TIMI 2 flow. He underwent a coronary stent placement. Subsequent post MI and arrest care was provided by the Cardiology Critical Care team including hypothermia protocol. Thirty-six hours later he was rewarmed, and made an excellent recovery without any neurologic sequelae. A few days later, he was discharged home in stable condition with a complete recovery.
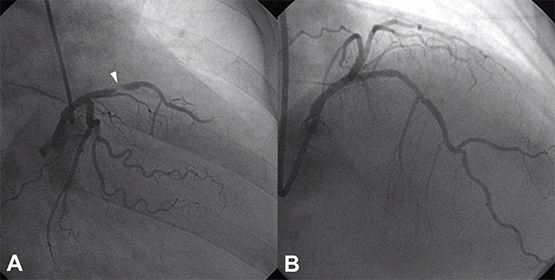
A: Coronary angiogram with tight 99% Mid LAD stenosis (white arrow). B: The same vessel after Transradial PCI.
Recently, the University of Cincinnati Medical Center was given the NCDR ACTION Registry-GWTG Platinum Performance Award by the American College of Cardiology Foundation for its commitment to improving care for heart attack patients.
“We have worked very hard on bringing our heart attack (myocardial infarction) program at the University of Cincinnati to the highest standards. This reflects better patient outcomes as we see in this case,” says Tarek Helmy, MD, professor of cardiology, and Medical Director of the Cardiac Catheterization Laboratory.
REFERENCES:
1.Rao SV, Ou FS, Wang TY, Roe MT, Brindis R, Rumsfeld JS. Trends in the prevalence and outcomes of radial and femoral approaches to percutaneous coronary intervention: a report from the National Cardiovascular Data Registry. JACC Cardiovasc Interv. Aug 2008;1(4):379-86. [Medline].
2.Bertrand OF, Rao SV, Pancholy S, Jolly SS, Rodes-Cabau J, Larose E. Transradial approach for coronary angiography and interventions: results of the first international transradial practice survey. JACC Cardiovasc Interv. Oct 2010;3(10):1022-31. [Medline].
3.Caputo RP, Tremmel JA, Rao S, Gilchrist IC, Pyne C, Pancholy S. Transradial arterial access for coronary and peripheral procedures: Executive summary by the transradial committee of the SCAI. Catheter Cardiovasc Interv. Nov 15 2011;78(6):823-839. [Medline].
4.Feldman DN, Swaminathan RV, Kaltenbach LA, Baklanov DV, Kim LK, Wong SC. Adoption of radial access and comparison of outcomes to femoral access in percutaneous coronary intervention: an updated report from the national cardiovascular data registry (2007-2012). Circulation. Jun 11 2013;127(23):2295-306. [Medline].
 Imran Arif, MD, FSCAI, FACC
Imran Arif, MD, FSCAI, FACC
Professor of Clinical Medicine
Interventional Cardiology
University of Cincinnati College of Medicine
Medical School: King Edward Medical College
513-558-6890
imran.arif@uc.edu
Leave a reply →