
Voice/Swallowing Database: Promoting Better Patient Outcomes and Getting Ahead of the Value Curve
Establishing quality improvement measures is the impetus for a clinical database for the Voice and Swallowing Center at the University of Cincinnati (UC) Medical Center. The national move to physician quality reporting systems (PQRS) requires establishment of outcome measures for physician and practice audits, as well as future incentive payments and penalties. According to Rebecca Howell, MD, assistant professor of otolaryngology, “In June 2016 the American Academy of Otolaryngology-Head and Neck Surgery launched Regent ENT Clinical Data Registry, the first national database for otolaryngology-specific data. Our hope is that the national organization may look to UC Medical Center for our laryngology-specific measures and standards in voice and swallowing disorders.”
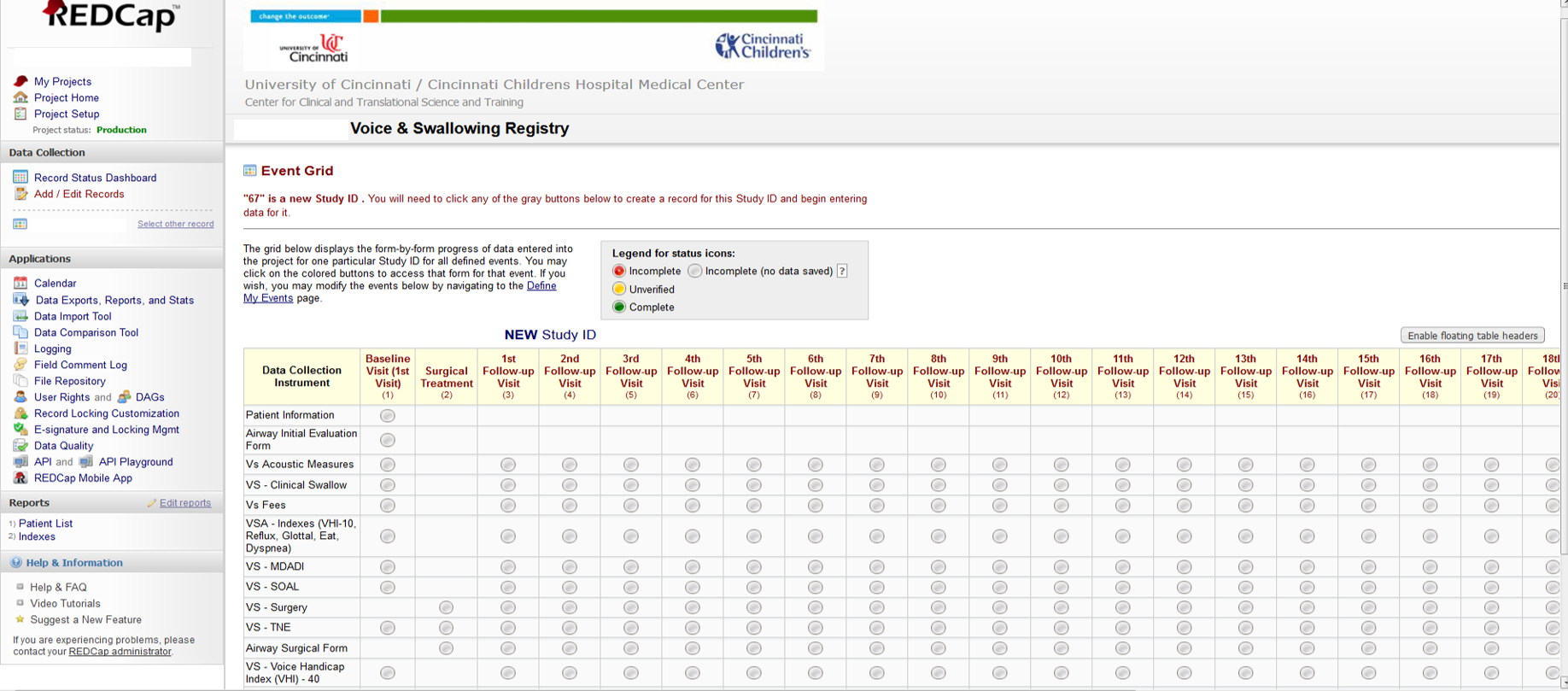
A screen shot of the clinical database for the Voice and Swallowing Center at the University of Cincinnati (UC) Medical Center.
Image courtesy of Rebecca Howell, MD.
In 2014, Dr. Howell began collaborating with Sid Khosla, MD, associate professor of otolaryngology, and assistant professor Bernice Klaben, PhD, CCC-SLP, who began the database initiative in 2012. As Dr. Howell explains, “It takes a long time to design a database, particularly in deciding how much data are needed and relevant.” After she and her colleagues had agreed on templates, standardized instrumental exams, notes, and order sets, the database launched in March 2016. Since then 1,112 patients have been enrolled, which Dr. Howell terms “an excellent volume.” With this system, she explains, physicians in the Voice and Swallowing Center “will learn what we do well and what we can improve upon.”
Included in this database are five validated patient questionnaires (fewer than 10 questions each) that are used in pre-treatment planning and post-treatment evaluations: 1) EAT-10, dysphagia index; 2) VHI-10, voice handicap index; 3) GFI, glottal function index; 4) DI, dyspnea index and 5) RSI, reflux syndrome index. “Because these questionnaires have been validated, we know they work,” says Dr. Howell, “and we will be able to quantitatively track outcomes and learn who has improved, how much, and if it was with surgery, therapy or medical treatment.”
Several patient cohorts have been identified for specific study. This summer, Dr. Howell and her colleagues began looking at patients with Parkinson’s disease because there is a large spectrum in voice and swallowing complaints that are non-responders to the current standard of care, speech therapy (Lee Silverman Voice Therapy, a Parkinson-specific treatment). Additionally, Dr. Howell, Dr. Khosla, and their newest laryngology partner, John Paul Giliberto, MD, will examine surgical outcomes, by studying pre-operative data, as well as surgical results, to determine which procedures were successful. “In which patients did we do well? What were the differences, and what is their clinical meaning? These are some of the questions we’ll address,” says Dr. Howell. She and her colleagues are also thinking beyond their practice: eventually, to contribute to a national registry such as the Regent ENT Clinical Data Registry, which allows other institutions to access prospective data, identify trends, and improve patient health.
These efforts are part of a nationwide trend in medicine. “We will start being scrutinized for outcomes, and it’s always better to generate ideas and meaningful data pertinent to our specialty,” says Dr. Howell.
Another impact of the PQRS impetus is cost, which can be addressed only after safety and efficacy are assured, says Dr. Howell. Cost – both payments and penalties – is a significant issue in any PQRS discussion.1 She described the trend toward in-office procedures in laryngology performed under topical anesthesia alone (e.g., KTP laser treatment, transnasal esophagoscopy, transnasal esophageal dilations, and injection augmentation for vocal folds). “Studies have shown these procedures can be performed, in appropriate patients, safely and effectively, in the office.2 If we demonstrate good outcomes and benefits that are consistently similar to those performed in the operating room, we can look at these nationally and should start talking about cost,” says Dr. Howell.
Dr. Howell has advice for physicians thinking about implementing a database: “The biggest issue is identifying one to two outcome measures that are useful for your practice and dedicating your time to consistently tracking them. It is important to be very specific, as well as minimizing the time that it will take physicians and patients to enter data – five minutes maximum,” Dr. Howell says.
References
1. PQRS wizard and CMS quality initiative. American Academy of Otolaryngology-Head and Neck Surgery. Available at: http://www.entnet.org/content/physician-quality-reporting-system-pqrs. Accessed July 10, 2016.
2. Young VV, Smith LJ, Sulica S, Krishna P, Rosen CA. Patient tolerance of awake, in-office laryngeal procedures: a multi-institutional perspective. Laryngoscope. 2012;122:315-321.
Additional Reading
Cohen WA, Gayle LB, Patel NP. An algorithm for building an electronic database. Available at: http://www.eplasty.com/index.php?option=com_content&view=article&id=1542&catid=15&Itemid=116. Accessed July 10, 2016.
 Rebecca J. Howell, MD
Rebecca J. Howell, MD
Assistant Professor of Otolaryngology
Phone: (513) 558-4564
Email: howellrb@ucmail.uc.edu
Connect with Dr. Howell on Doximity
Leave a reply →