
EKOS Offers Great Benefits for High-Risk Pulmonary Embolism Patients
The EkoSonic Pulmonary Embolism (EKOS®) System is “so effective, even for the most complex cases, that it’s hard not to use it for all patients with pulmonary embolism [PE],” says Timothy Smith, MD. Dr. Smith, an interventional cardiologist, is director of the cardiovascular ICU and assistant professor of medicine at the University of Cincinnati Medical Center (UC Medical Center). He is one of only a few interventional cardiologists in the country to be trained and board certified in interventional cardiology and critical care medicine.
 EKOS1 uses a catheter system to deliver clot-busting medicine directly to the embolism, at the same time using ultrasound energy to loosen the clot and allow the drug to permeate the clotting strands, increasing the thrombus surface area and letting the drug reach more plasminogen activator receptor sites. The use of ultrasound permits a lower but equally effective drug dosage. Compared to other endovascular techn
EKOS1 uses a catheter system to deliver clot-busting medicine directly to the embolism, at the same time using ultrasound energy to loosen the clot and allow the drug to permeate the clotting strands, increasing the thrombus surface area and letting the drug reach more plasminogen activator receptor sites. The use of ultrasound permits a lower but equally effective drug dosage. Compared to other endovascular techn
iques to treat PEs, EKOS reduces treatment time and the lytic dose, ultimately lowering cost and the risk for related bleeding complications.
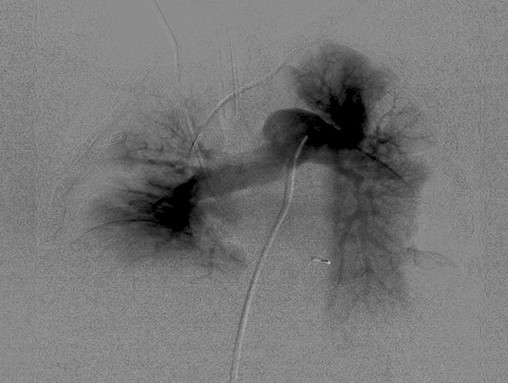
This pulmonary angiogram shows a bilateral PE.
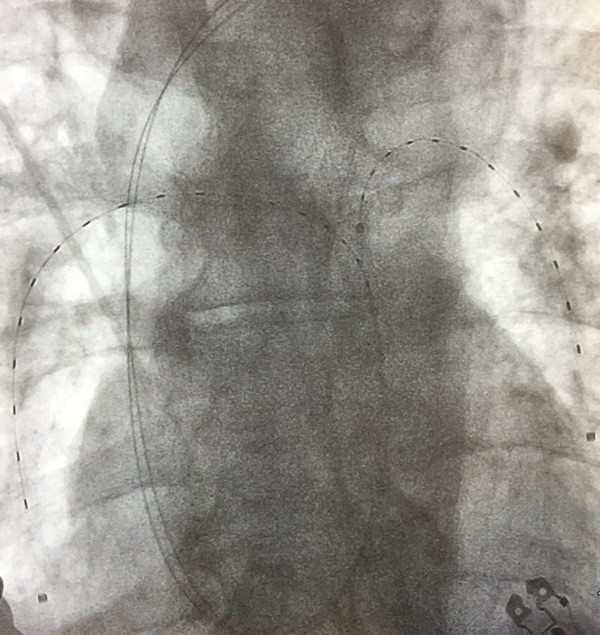
Two EKOS catheters are in place, one in each lung, during the treatment of a PE. Images courtesy of Timothy Smith, MD.
Dr. Smith anticipates that national data from the OPTALYSE trial will be published within six months and will demonstrate that significant hemodynamic improvement occurs at roughly six hours suggesting that perhaps the infusion time and dose of thrombolytic can be cut in half instead of the typical 12 hours. While there is no goal for “door-to-catheter placement,” Dr. Smith estimates that from the time he receives a call about an EKOS candidate and assesses the patient to the time that catheters are in place is approximately 60 to 75 minutes. “It simply makes sense as time to treatment for any cardiovascular emergency suggests reduced morbidity and mortality,” says Dr. Smith.
At UC Medical Center, EKOS has delivered excellent results, even in patients who have experienced high-risk submassive and massive PEs. In the 30 cases in which EKOS was used in 2016, 15 patients had submassive PEs and 15 had massive PEs. The patients ranged in age from 33 to 85 years old, with the mean age being 68 years old. None of the UC Medical Center patients who underwent EKOS experienced intracranial bleeding, “which is the complication that worries us most in PE patients receiving systemic thrombolytics,” says Dr. Smith. “We’ve had great success in high-risk populations, such as postoperative patients, intracranial and subdural bleeding as well as patients who have experienced recent trauma or undergone spinal surgery. This is truly remarkable when the additional bleeding risks for these patients are extremely high.”
“With the exception of one patient, who suffered profound anoxia and died as a result of withdrawal of care at the family’s wishes, 29 of the 30 were alive and well at discharge,” Dr. Smith says. He calls these results “a little unusual, both because the mortality rate was so low and the fact that UC Medical Center team has performed as many massive EKOS procedures as submassive. In contrast, only 25% of PE subjects in the two EKOS trials had massive PEs.”2,3 Dr. Smith estimates that 66% of the PE patients who received EKOS treatment at UC Medical Center would have been excluded in similar trials, and would have been treated with IV medications to break up the clots. He anticipates publishing UC Medical Center’s EKOS results.
One reason for UC Medical Center’s notable successes, Dr. Smith says, is a coordinated, experienced team of cardiac and endovascular interventionalists, critical care physicians, cardiac surgeons and cath lab personnel who are available 24 hours/day, 7 days a week. “This UC Medical Center team, the only one of its kind in the Cincinnati region, has multiple levels of training and has developed the willingness and the expertise to treat our high-risk PE patients,” he says.
View this video to see how EKOS treatment impacted this patient.
References
1. EkoSonic Pulmonary Embolism (EKOS®) System_https://www.btg-im.com/EKOS/US/
2. Kucher N, Boekstegers P, Müller OJ, et al. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation. 2014;129:479-486.
3. Piazza G, Hohlfelder B, Jaff MR, et al; SEATTLE II Investigators. A prospective, single-arm, multicenter trial of ultrasound-facilitated, catheter-directed, low-dose fibrinolysis for acute massive and submassive pulmonary embolism: the SEATTLE II study. JACC Cardiovasc Interv. 2015;8(10):1382-1392.
Timothy Smtih, MD
Timothy Smith, MD
Interventional Cardiologist
Director, Cardiovascular ICU
Assistant Professor of Medicine
PHONE: (513) 475-8521
E-MAIL: smith5ty@ucmail.uc.edu
Connect with Dr. Smith on Doximity
Leave a reply →